The Darker Side of Being an Aid Worker
A few days ago I read an IRIN article by Ben Parker, Memento Mori, on humanitarian aid work and the risks aid workers face in conflicts. Aid agency managers accept the organizational risks of operating in conflict areas; we, as individual aid workers, accept the personal risks. But the risks go way beyond being killed or wounded; there are risks we never really talk about.
The statistics of aid worker casualties affected by attacks is horrific: 2,913 nationals and 544 internationals since 2000.
Every time I hear of an attack on aid workers, I say to myself “there but for the grace of God go I.” Even though I am agnostic, this 16th century saying resonates with me. After 15 years of aid work it is no longer remarkable that I know friends and colleagues that have been killed or wounded. Sadly it is unavoidable; there will be more. Our fate is not entirely in our hands.
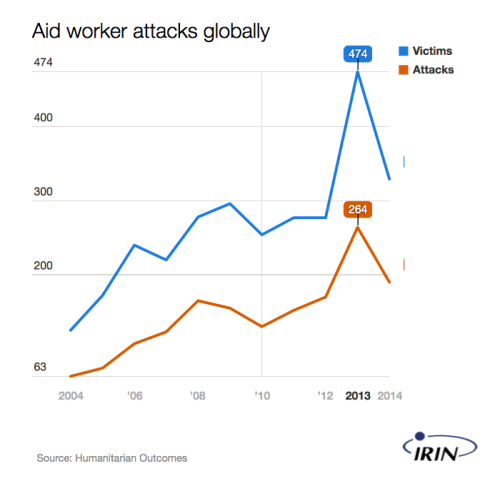
IRIN, Fewer aid worker attacks. That’s good, right?, 13 July 2015
Hidden behind the horrific casualty statistics are the families of aid workers killed or wounded. What happens to them? Who are they? Where are they? I believe that many of them simply disappear from our collective consciousness. Although I don’t have any data to support my belief, I assume that many aid workers who are harmed, especially nationals, don’t have life insurance, medical insurance, or invalidity coverage. If they do, I doubt it is adequate.
A few years ago a well-meaning colleague came into my office with a yellow envelope asking for a donation for a UN contractor who had been killed in a terrorist attack. Contractors are not insured, hence the envelope. I was told that he had a wife and a couple of young children. I was aghast. On one hand I was glad that we were doing something; on the other hand I was stunned. Really? The welfare of a widow and her children depended - in part - on my generosity, a UN staff member half a world away.
There are other concealed numbers behind the casualties that we don’t talk about enough. What happens to the thousands of aid workers who are exposed to the stress of humanitarian work; bearing witness to the horror of man’s inhumanity? For every aid worker casualty, there are many near misses. Many of us have escaped harm by simply being in the right place at the right time, rather than being in the wrong place at the wrong time. Not always exposed directly to the trauma of conflict, aid workers experience it through their daily work. The trauma is transferred from the victim to ourselves. Walls are built; emotions are suppressed.
For me, the rote mantras of: drink less, don’t smoke, exercise more, and my favourite of recent years, “have you tried yoga” don’t work for me. If we are honest, we know that as a system what we do for the mental health of aid workers is woefully inadequate.
The Antares Foundation recently put forward that around 30% of aid workers report significant symptoms of post-traumatic stress disorder (PTSD) upon returning from assignment. A 2013 study by UNHCR showed that 47 percent of surveyed staff stated they had experienced difficult sleeping in the previous month. More alarming, 57 percent reported symptoms consistent with depression.
Other studies show that approximately 80 percent of national aid workers experience symptoms of distress, and that 3 to 7 percent find that the symptoms interfere with their performance. A 2012 study of national humanitarian aid workers in northern Uganda by the International Society for Traumatic Stress Studies revealed that over 50 percent of workers experienced 5 or more categories of traumatic events. Although the authors of the report did not conduct clinical exams, data indicated that 68 percent, 53 percent, and 26 percent of respondents reported symptom levels associated with high risk for depression, anxiety disorders, and PTSD. I am not aware of similar studies, but I believe it is reasonable to assume such findings would be replicated in other emergency contexts.
Drawing on extensive studies over the past 50 years on the post-traumatic stress soldiers’ experience, we know that post-traumatic stress can be cumulative and manifest itself many years later. Aid workers can experience similar levels of stress, but without the benefits of the training or support networks many militaries provide (and even they fall short). Unlike most militaries and emergency services around the world, there is rarely, if ever, psychological testing of aid workers before they deploy to humanitarian emergencies or when they return.

An armed militiaman, Tripoli, 20 October 2011. Aid workers are often confronted by irregular militias in their line of work. © Brendan McDonald
Before I went to Iraq last year my high blood pressure and vaccination card were checked; no one asked if I was mentally fit. Instead I voluntary went to see my General Practitioner, someone I trust. There is no systematic approach to the mental health of aid workers or acknowledgment of the stress aid work places on an individual. We never talk about self-harm or suicide rates amongst aid workers. Does the data even exist?
A friend of mine, who was wounded in an incident a few years ago in Africa, told me how isolated and alone they felt after the attack. There were no personal messages from senior managers at headquarters; no acknowledgment of what they had gone through. When seeking confidential advice about how to deal with post-traumatic stress, they were advised not to tell anyone, and to make sure that their medical certificate was from a General Practitioner, not a Psychiatrist. Better to be hurt on the outside, where people can see it, not on the inside. Sadly this story is not an isolated one; post-traumatic stress, depression, burnout, and breakdowns are a very real part of being an aid worker. When I experienced burnout a few years, I did not tell my employer. I felt at the time it would have been the death of my career; much better to have leukaemia.
To be fair, it is not as though the humanitarian sector has been idle when looking at issues relating to the health, safety and security of aid workers. Some aid agencies do make an effort, but recent research has found that:
“Some aid workers feel the support options offered to them are either inadequate (time-limited or inaccessible), ill-fitting (the available clinicians or programmes offered don’t understand or tackle the issues faced) or unsafe (they fear that a call for help could result in professional blemishes on personnel records).” … “Others believe support offered, like a list of self-care tips or brief rest and relaxation, is too simple."
Rich McEachran, “Aid workers and post-traumatic stress disorder,” The Guardian, 3 March 2014
The emergence of specialist NGOs, such as the Mandala Foundation and MINDFULNEXT, is a proxy indicator of the need for more resources for mental health. People in Aid, a 20 year old not-for-profit membership organization, has been advocating, supporting and recognizing good practices in the management of aid workers. The 7th principle of the People in Aid Codestates that “we have a duty of care to ensure the physical and emotional well-being of our staff before, during and on completion of their period of work with us.”
Since the Code was first developed, ten organizations have been verified compliant in the People in Aid Code; a further 40 have a “desire to continuously improve their HR and people management skills.” Given the number of aid agencies across the world, which must number in the thousands, the low level of commitment to the People in Aid Code is a shocking indictment of the system wide commitment to the welfare of aid workers, notwithstanding the few organisations who are endeavouring to live the code. The UN Secretariat, of which UNOCHA is part of, is not a member of People in Aid, nor do we subscribe to it. To OCHA’s credit, the Management Plan for 2014 - 2017 states that it "will implement staff-welfare policies and initiatives to identify and reduce stress levels, especially in work situations involving extensive exposure to physical and psychological hardship.” This is positive, but is it enough?
In the article Memento Mori Ben Parker asks the question, “How do you honour the sacrifices of aid workers without appearing to value them more than those they serve?”
Maybe the answer is to recognize that “people are central to the achievement of our mission”
Though I do not have all the answers, nor do I underestimate the challenges, here are six suggestions that are worth taking forward if we want to address this issue:
1. Come out of the closet. We must raise awareness and understanding of the importance of mental health for aid workers. Bring post-traumatic stress, depression, burnout, and breakdowns out of the closet. The welfare of aid workers, as well as those we seek to help, should be on the agenda of the World Humanitarian Summit. #ReShapeAid
2. Establish a Global Trust Fund for Aid Workers. We must move beyond the yellow envelope. We need to establish a fund to ensure that no matter what your contractual status, national or international, if you are an aid worker casualty, there is a safety net for you and your family.
3. Support the People in Aid Code. As a starting point, all humanitarian agencies, including the UN Secretariat engaged in humanitarian work, should commit to this code. This does not imply membership of the People in Aid organization, rather a genuine desire to meet minimum standards the code sets. It is mostly about a change in attitude, not additional expenses.
4. Enforce accountability for the Code. Pretty simple solution really; donors should only fund organizations committed to the code. Why would a donor fund an organization that doesn’t put people central to the achievement of their mission? Donors have a vicarious liability to ensure the agencies they fund do the right thing when it comes to staff welfare and safety.
5. United we stand, divided we fall. I know we don’t have a global aid worker union or association (now isn’t that a wonderful idea!), but collectively, as aid workers, we should demand our employers look after us. If they are not looking after us; we need to demand that they do.
6. Adopt a cycle of continous improvement. Keep the People in Aid Code alive and relevant; update it to reflect best practice and new knowledge. Principle 7 is a good starting point, but it can and should go much further.
In 2011, while living and working in the Palm City Compound in Tripoli with the rest of the UN family, the sound of celebratory fire was a constant. One on occasion the compound was attacked, the gun battle taking place about 100m from where my staff and I were sheltering in the hallway.
Selected articles on the mental health of aid workers:
Alessandra Pigni, Aid workers’ mental health: shouting into the wind, MINDFULNEXT, March 2012.
Colleen A. McFarlane, Risks Associated with the Psychological Adjustment of Humanitarian Aid Workers, The Australasian Journal of Disaster and Trauma Studies, 5 April 2004
Ellen Connorton*, Melissa J. Perry, David Hemenway and Matthew Miller; Humanitarian Relief Workers and Trauma-related Mental Illness, Oxford University Press, 8 September 2011.
IRIN, HEALTH: Aiding aid workers, IRINnews, 19 August 2010
Robert T. Muller, Mental Health Challenges Faced by Ebola Relief Workers, The Trauma & Mental Health Report, 13 February 2015.
Rosalie Hughesmarch, A Crisis of Anxiety Among Aid Workers, New York Times, 8 March 2015.
Timothy S. Paul, No Relief for Relief Workers: Humanitarian Aid Work Raises Risk of Depression and Anxiety, Columbia University, 1 October 2012.

An Equity T-Shirt by URevolution